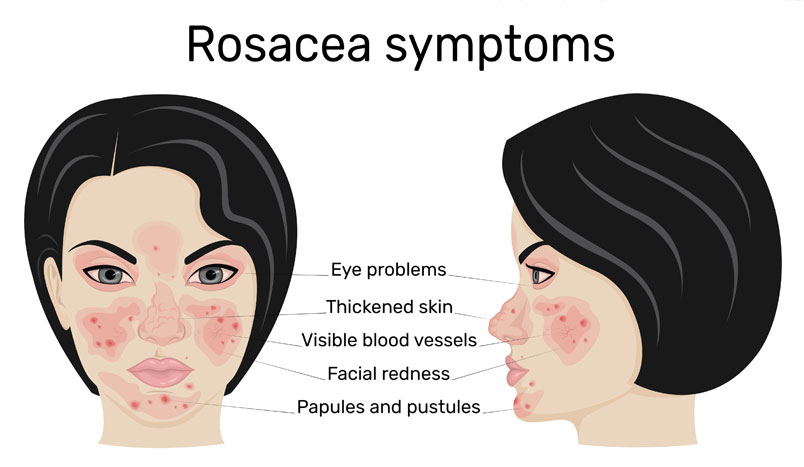
Rebecca Baxt, MD, medical director of BAXT CosMedical®, shared her dermatological expertise on the topic of ocular rosacea with Dermatology Advisor.1 The condition of ocular rosacea isn’t as well-know or understood as rosacea skin condition. Rosacea is a common chronic skin disease that starts with flushing and blushing. Subsequently, these episodes lead to the development of red lines called telangiectasia. Some patients may also develop pimples. This skin condition can be easily diagnosed and medically managed by a board-certified dermatologist. Furthermore, the visible symptoms can be improved cosmetically with laser and light source treatments.
On the other hand, ocular rosacea can develop in some people who have rosacea affecting their skin but with no symptoms of ocular rosacea, while others have ocular rosacea but no skin symptoms. Individuals can have both forms of rosacea. As with skin rosacea, there is no cure for ocular rosacea. Ophthalmologists can help control and treat symptoms.
Q: Is there anything patients can do to prevent rosacea from developing or worsening? What can be done to lessen the appearance of facial telangiectasias?
A: The answer is no, rosacea is genetic. Either you have it, or you don’t have it. There are some families and ethnicities where it is extremely common. I would say it is less common in darker skin types, but I have seen rosacea in all skin types. It is very common in fair-skinned people, particularly of Northern European descent, but there’s nothing you can do to prevent it from coming.
Common Rosacea Triggers
Once you have rosacea, there are ways you can prevent it from getting worse. Rosacea triggers include a variety of things, such as stress and weather changes. For example, some people get rosacea flares from wind, others get rosacea flares from sun. Additionally, people get rosacea flares from extreme heat in their face, so to the extent that you can control it, managing the temperature of the environment around you is helpful.
Foods are a big factor for rosacea on the skin. There is a whole list of foods that can trigger rosacea outbreaks, such as, hot foods, spicy foods, alcohol, nuts, chocolate, sometimes dairy, sometimes citrus. The food items are different for people, so I typically will give rosacea patients a list and have them check and say, “is this a problem for you?” You usually know within about a day or so of eating something. If every single time you have chocolate, you break out, well, then that’s a trigger for you, and you can reduce your rosacea by avoiding your triggers.
Another trigger is stress, but this is obviously harder to avoid. I always tell my patients, “I’d love to give you a prescription for no stress, and I’ll take that one, too!” To some extent you can learn to minimize your stress. Whatever that takes, whether it is exercise or meditation or walks in nature or getting good sleep, taking good care of your body, reducing the things that trigger your rosacea can prevent it from worsening.
I would also say to avoid hot water. I always tell patients with rosacea, things that make you red will make your face redder and redder and redder, so washing your face in hot water is always a bad idea. I always recommend cool water. Scrubbing your face is a bad idea, so mild cleansers, fingertips, cool water, these are things to help prevent it from getting worse.
Interestingly, ocular rosacea symptoms can be triggered by the same factors as skin rosacea. Ocular rosacea is viewed a chronic condition that is treated with medication by an ophthalmologist. (To learn more about ocular rosacea treatment, read the article, “With Ocular Rosacea, Two Clinicians Are Better Than One.“)
Q: What over-the-counter options can patients use to manage facial telangiectasias and erythema?
A: I would say there are three main things to do for those. One, in the last number of years, we’ve gotten creams that are prescriptions that are — the brand names are Mirvaso® and Rhofade®. They are vasoconstrictors, so if you have health insurance, and your insurance company will cover them, you can use those creams every morning, or if you’re going to a special event in the evening, and it will give you a certain amount of relief — 6 hours, 8 hours, whatever it may be. The problem is, they’re very expensive, a lot of people don’t have health insurance, and insurance companies often don’t cover it, because while we know rosacea is a medical condition, a lot of insurance companies feel that the erythema and the flushing and the blushing is a cosmetic issue.

*Actual patients. Results may vary and are not guaranteed.
See Dr. Baxt’s before and after photos of rosacea patients
So, if you can get those creams, they can be very helpful on a temporary basis. The things that are more helpful on a more long-term basis are lasers and intense pulsed light treatment. There are a few different types of lasers. Pulsed dye lasers, KTP lasers, any laser that works on red things. Usually, it is the hemoglobin in the blood vessel, and the laser energy gets absorbed, it damages those blood vessels, and then your body heals and reabsorbs those damaged vessels.
It does usually take more than one treatment. It can cause a little bit of discomfort. It can cause swelling, occasionally bruising. There is Intense Pulsed Light (IPL), which is a little bit gentler than the lasers. It is multiple wavelengths, instead of just one wavelength like a laser, and the IPL also can reduce redness. It is also absorbed on a similar spectrum to the lasers, it’s just a little bit milder, so I find that IPL works a little bit better for background erythema, background redness, flushing, and blushing, and that the lasers will work better on individual larger blood vessels. Many of my patients will do a combination of both of those treatments.
Q: When dermatologists perform Intense Pulsed Light therapy for facial rosacea, are they including the eyelids?
A: We do not, as dermatologists. When we are doing Intense Pulsed Light, we really are very, very careful to shield the eyes, because one of the side effects of laser and light treatment can be eye damage. I have never seen it in my office, because we take eye protection very seriously, so we are all wearing special goggles, and the patient is wearing eye shields, so we do not treat the eyelids at all in my practice, and in most dermatology practices.
IPL rosacea treatment
In order to treat the eyelids, I feel that the person probably needs eye drops to anesthetize the eye, and an internal eye shield, which there are some dermatologists, probably, who would do that. I am not one of them, but this is a good example where there could be improved cooperation between the two specialties: dermatologist and ophthalmologist. I wouldn’t feel comfortable doing that, so we shield the eyes and we do not treat the eyelids, but we treat the rest of the face.
Q: Are oral tetracyclines the best — or only — approach, or do other oral drug classes meaningfully help with facial rosacea?
A: For rosacea, tetracyclines really do work incredibly well. The one that we typically use is doxycycline — 50 mg, 100 mg, maximum dose would be 100 twice a day. Sometimes, we will use a very, very low dose, like a 20-milligram twice a day, or even a 40-milligram long release once a day, so doxycycline, which is a tetracycline, works really well, but it has two main problems.
I advised my patients that doxycycline can cause GI and stomach upsets. I recommend that patients take it with food and be cautious of sun exposure as antibiotics can cause sun sensitivity, which is a real issue for fair-skinned patients, especially certain seasons, or especially in certain areas, if you live in a sunny place, so sometimes, doxycycline is not optimal. Ophthalmologists often recommend this specific antibiotic for ocular rosacea.
My second line therapy would be minocycline, which is a cousin of doxycycline, which is also a tetracycline, but it has much less GI upset and much less sun sensitivity. However, minocycline can have other side effects. Obviously, anyone can be allergic to any of these drugs, but if doxycycline is not working well or is not optimal for that patient, my second line would be minocycline, which is again, a tetracycline.
There are other antibiotics that are used but they typically don’t work as well. If someone is allergic or cannot tolerate the tetracyclines and they need an oral antibiotic, I will sometimes use Bactrim®. Bactrim® is a cheap, very effective generic available antibiotic. It is not that popular, because it can cause severe allergic reactions, but again, if someone doesn’t have health insurance, and they need something inexpensive, or they cannot tolerate tetracyclines, Bactrim® would be another option. I don’t use it very often, but I would say yes, there are other options if a patient cannot tolerate a tetracycline.

Q: How can dermatology and optometry be more collaborative in managing ocular and facial rosacea?
A: Doctors of all specialties and other healthcare professionals really just need to take the time to pick up the phone and call each other. It’s very difficult in the busy day of a healthcare professional to find the time to call another medical practitioner, but that’s really what I think needs to happen on complicated cases and difficult management issues of patients. So, yes calling and discussing the patient is the best way be more collaborative.
I will sometimes send notes to another medical professional. I keep a blank pad in all my exam rooms with my practice name and phone number and website so that I can easily write a note and have the patient give it to their doctor to make sure that they return my phone call or send me a note back. For my patients who were referred by a doctor, I will send them a consultant note, where some people will send a copy of their note and report, so it needs to be communication, whether it’s a phone call, whether it’s sending something through snail mail. Sometimes, maybe email, you know, if you’re working in a large healthcare system and everybody can see each other’s notes, because they’re all on the same electronic medical record, that becomes much easier to see and message somebody, but for those of us in private practice, that doesn’t usually happen, so it requires a phone call or a note.
1Weidmayer, OD, S. (2022, June 13). Rebecca Baxt, MD: “With Ocular Rosacea, Two Clinicians Are Better Than One.” Dermatology Advisor.
